Stay Informed
"*" indicates required fields
Blog

Medicaid Myth Busting
With the recent passage of the “One Big, Beautiful Act” (OBBA), Medicaid has been all over the news lately.
Unfortunately, a great deal of misinformation encircles this debate. As Pennsylvania lawmakers debate the state budget, it’s of the utmost importance that we dispel some of the most pernicious myths surrounding Medicaid.
Myth: The OBBA slashed Medicaid spending.
Fact: Medicaid will continue to grow but at a slower rate.
“Pennsylvania got screwed,” Gov. Josh Shapiro recently told a crowd in York, citing his dubious claims about how the bill “slashed Medicaid.”
Contrary to the governor’s claim, Medicaid will still grow. Undoubtedly, the program’s baseline will shrink when OBBA goes into effect. However, the Congressional Budget Office found that federal Medicaid spending will still grow by 50 percent over the next decade. OBBA simply slowed the growth of Medicaid.
Only in the world of politics can a multibillion-dollar spending increase be called “a cut.”
Myth: Medicaid’s new work requirements are onerous.
Fact: The OBBA work requirements are minimal.
The OBBA requires recipients to perform 80 hours of work or other qualifying activities (e.g., job training, community service) for one in every three months.
Not 80 hours per week.
Not 80 hours per month.
Instead, 80 hours per one in every three months. At a bare minimum, that requirement translates into 320 hours in a year—less than 1 percent of a traditional full-time equivalent.
Respectfully, Medicaid work requirements are a low hurdle to jump.
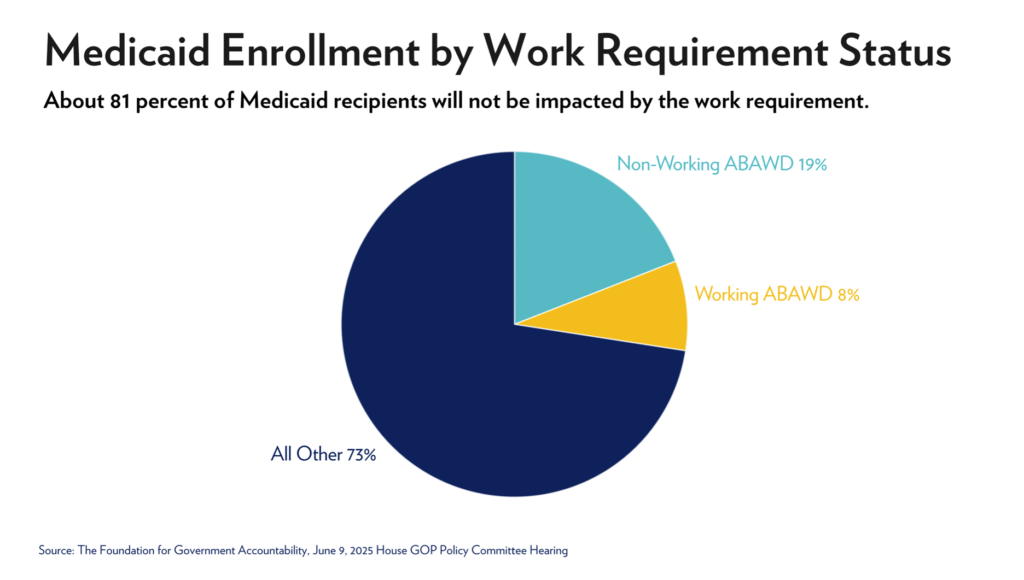
Myth: Work requirements will negatively impact Medicaid recipients.
Fact: Work requirements return recipients to the workforce and help them secure better private coverage.
The new work requirements won’t affect about 81 percent of Medicaid recipients in Pennsylvania.
Experience shows that working-age enrollees benefit from work requirements. Arkansas became the first state to require part-time work for able-bodied, childless adults on Medicaid in 2018.
The Arkansas law required similar work requirements to OBBA: Enrollees ages 19–49 must perform 80 hours of work or other qualifying activities (e.g., job training, community service) per month. (That works out to 960 hours per year—about 5 percent of a full-time equivalent.)
Importantly, Arkansas’s plan worked—quite literally. According to state-level data, more than 9,200 Medicaid enrollees gained employment after the work requirements went into effect. Plus, more than 14,000 Arkansans left the program because their income levels increased.
In the end, Medicaid recipients will become more financially independent and less reliant on government subsidies.
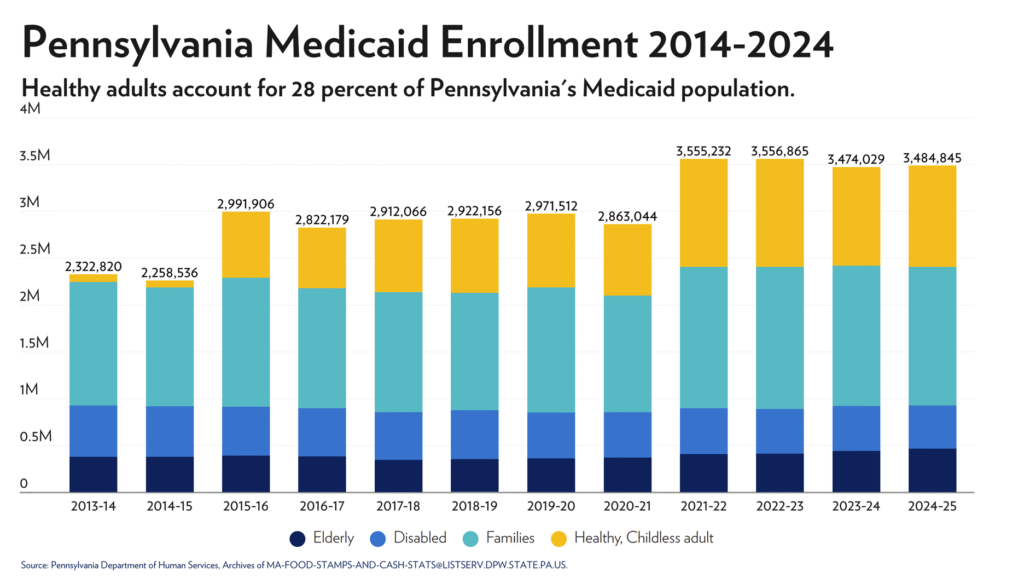
Myth: Most healthy, able-bodied Medicaid enrollees already work.
Fact: About half do not work.
Some reform opponents argue that work requirements are unnecessary because most healthy, able-bodied enrollees already have jobs.
However, this claim is based on self-reported data, which is far from reliable. For example, a 2022 survey found that 30 percent of Medicaid enrollees mistakenly reported that they weren’t enrolled in Medicaid.
Meanwhile, state-level data tends to be more reliable. Today, Pennsylvania enrolls about 800,000 working-age adults in Medicaid. The Pennsylvania Department of Human Services found that about half of this group is employed.
Myth: More than 310,000 Pennsylvanians will lose their Medicaid coverage.
Fact: This number assumes that able-bodied recipients will be unable to meet the newly established requirements for part-time work, volunteer, or education enrollment. As noted earlier, work-to-welfare programs have proven successful in other states, such as Arkansas.
Several Pennsylvania politicos, including Shapiro, have recently cited this misleading figure. But the number lacks merit.
Meanwhile, the new work requirements will not affect coverage for Medicaid’s most needy recipients: low-income kids, seniors, individuals with disabilities, etc. In fact, these reforms protect Medicaid for the most vulnerable populations.
Myth: Hospitals, especially those in rural communities, will close.
Fact: Moving patients to private insurance programs is the best way to address fiscal challenges that rural hospitals already face. Plus, the new act established a $50 billion fund for rural hospitals.
Medicaid pays significantly less than private insurance for the same medical care. In Pennsylvania, Medicaid paid hospitals 82 cents for every dollar spent by private insurance for inpatient care. That reimbursement rate is even lower in rural communities: about 74 cents on the dollar.
Work requirements that result in more Pennsylvanians working with access to private insurance are far better for rural hospitals than expanding the number of patients reliant on an underpaying government program.
Most importantly, the OBBA also established a $50 billion grant program for rural hospitals. Last year, rural hospitals received about $12 billion in Medicaid funds, so this new grant program could potentially quadruple those returns.
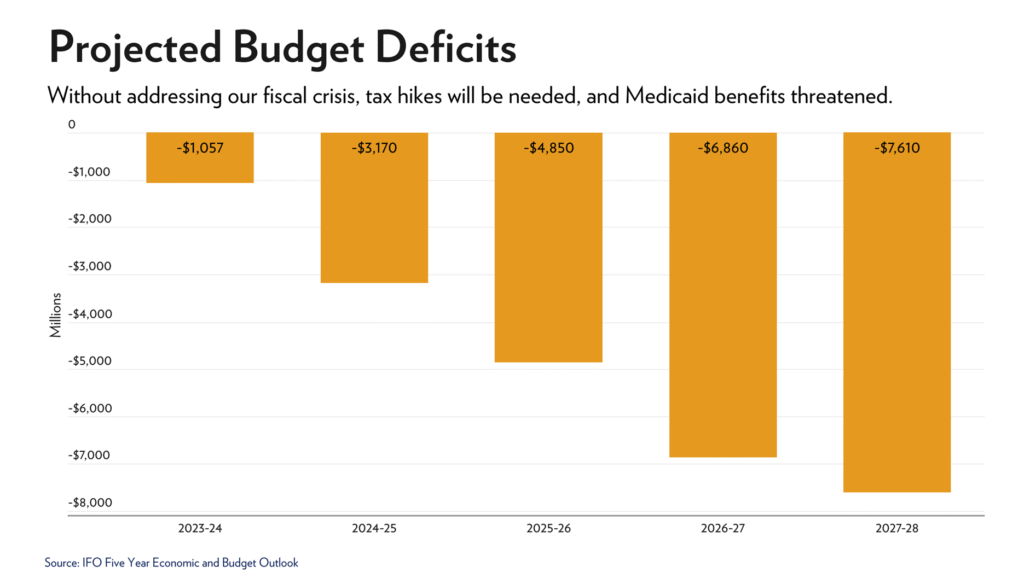
Myth: Now is not the time for Pennsylvania to address Medicaid reform.
Fact: Pennsylvania faces a significant budget deficit, and Medicaid is the commonwealth’s largest expense.
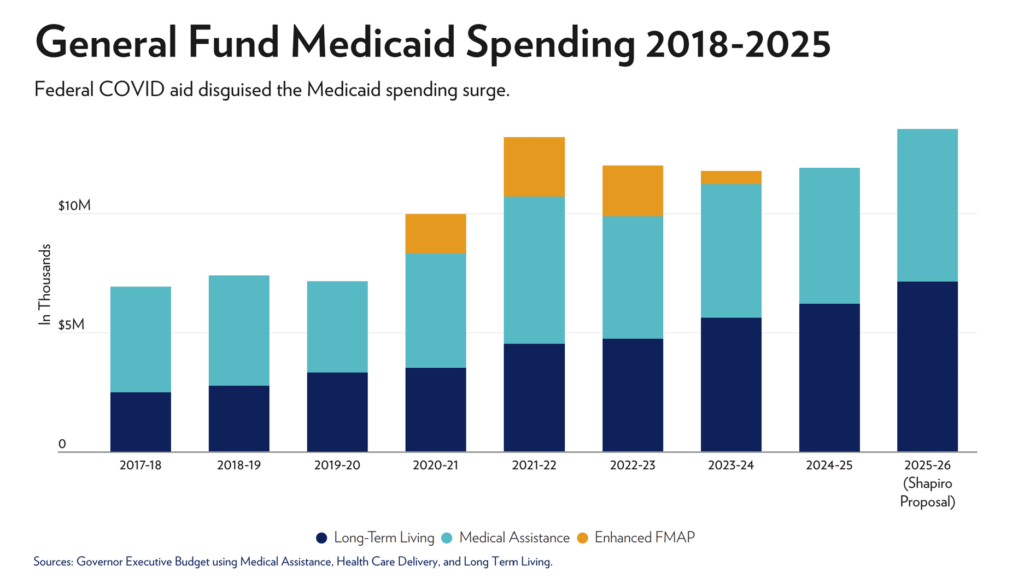
Medicaid is a huge expense for Pennsylvania.
Spending on Long-Term Care alone is projected to grow 3 times faster than overall revenue in the next 5 years. Pennsylvania’s Independent Fiscal Office projects total Medicaid spending to reach $54 billion in fiscal year 2025–26—about one-third of general fund spending. Plus, for the past six years, Medicaid spending has increased by 8 percent annually and is projected to rise by 9 percent next year.
Considering that the commonwealth’s projected revenue will grow by only 1 percent next year, the long-term expense of Medicaid is unsustainable. Pennsylvania cannot afford not to address Medicaid.
Myth: Medicaid reforms are unpopular.
Fact: A significant majority of Pennsylvanians support these commonsense reforms.
In 2018, two-thirds of Pennsylvanians supported work requirements for working-age, able-bodied Medicaid enrollees without dependents. Seven years later, that robust majority grew to 84 percent.
And this sentiment isn’t limited to the Keystone State. A separate national poll found the exact same percentage of support.
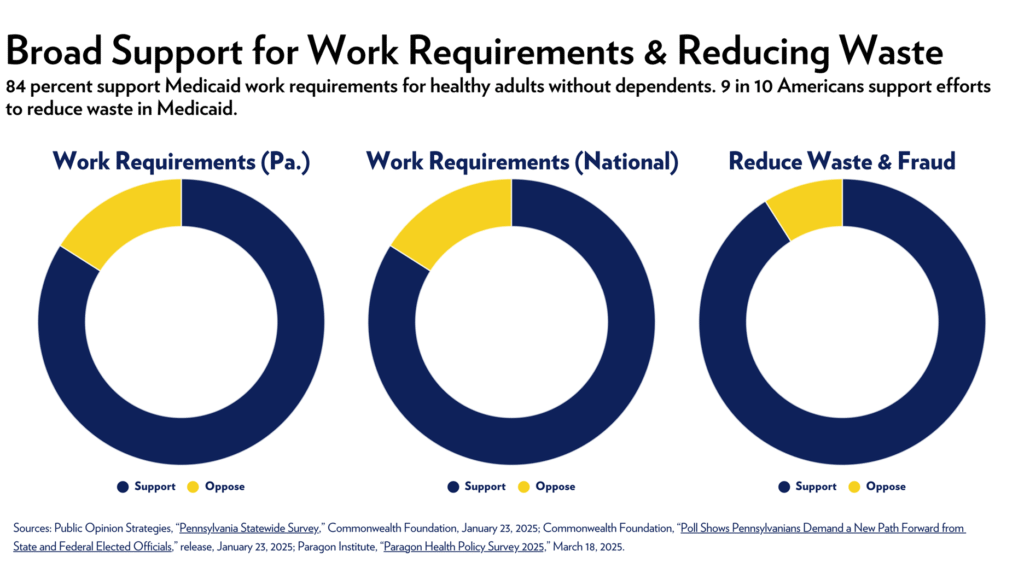
Myth: Medicaid doesn’t have an issue with waste, fraud, or abuse.
Fact: Medicaid wastes billions of dollars on wrongful payments.
Federal prosecutors recently filed charges against a Pennsylvania woman for nearly $1.1 million in fraudulent Medicaid reimbursements.
Sadly, this isn’t an isolated incident.
Over the last decade, the federal government paid as high as $1.1 trillion in improper Medicaid payments. In Pennsylvania, improper payments totaled $2.3 billion. Recently, the Pennsylvania Auditor General found incorrect payments in 12 percent of the audited cases.
Given Medicaid’s already large budget and the sizable waiting list for services for the state’s disabled population, Pennsylvania should take action to address waste, fraud, and abuse.
Ultimately, Medicaid is a broken system—and it has been for a long time. Without reforms, taxpayers will continue to subsidize its inefficiencies and pass along this unsustainable financial burden to the next generation to shoulder.
Connect With Us
Email Sign Up
"*" indicates required fields